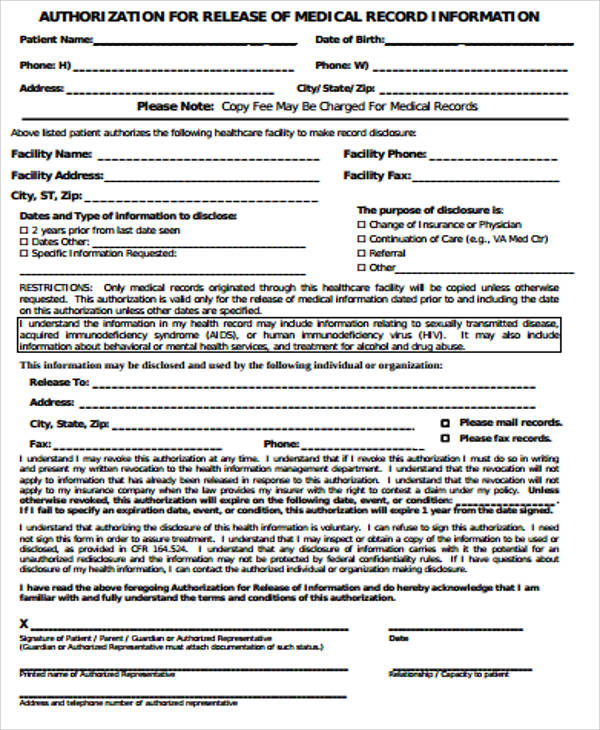
Patient Authorization Form To Release Medical Records. Follow these steps to complete the form: Enter the patient name (maiden or former name If patient had testing, diagnosis or treatment for any condition(s) as described under the SPECIAL AUTHORIZATION sections, it is required that. Use the first blank line in this section to name the individual (Disclosing Party) who will be authorized to release the Patient's medical records through this paperwork and the Health Insurance Portability And Accountability Act.
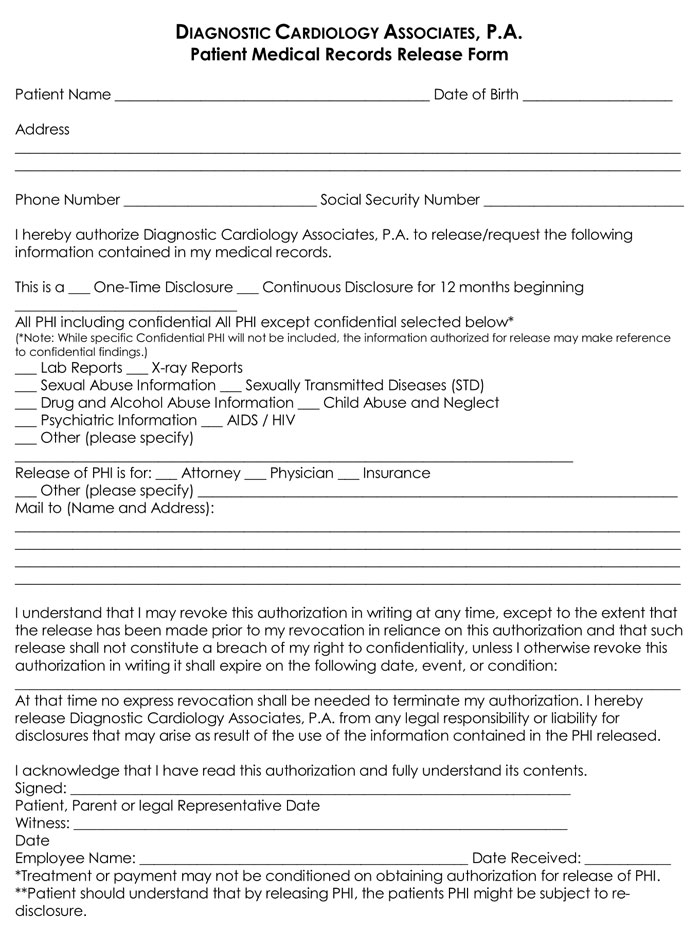
This form is to request a client's medical records.
I may inspect and receive a copy of the information to be used and disclosed pursuant to this Authorization form.
20+ Samples of Medical Records Release & Authorization Forms

Release of Records Authorization | Sleep Medicine Center

27 Printable Generic Authorization Medical Release Form ...
MEDICAL RECORDS RELEASE AUTHORIZATION in Word and Pdf formats
30+ Medical Release Form Templates ᐅ TemplateLab
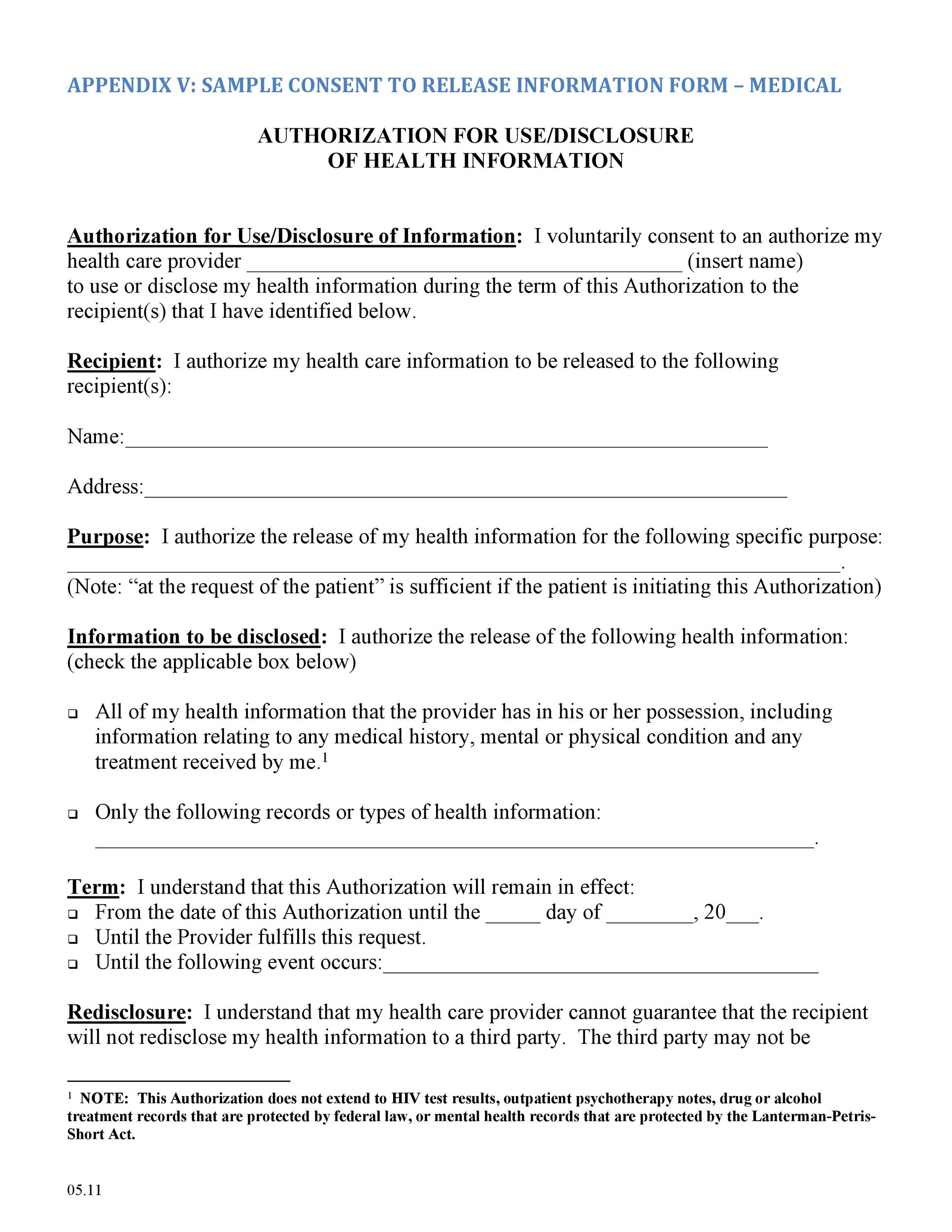
HIPAA Patient Consent & Authorization For Release of PHI
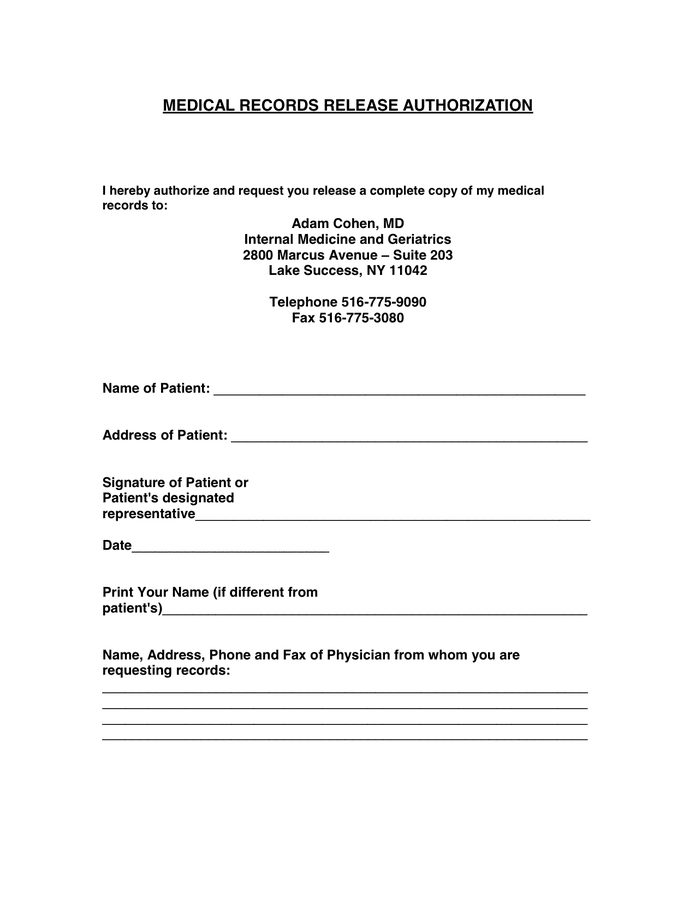
LETTER OF AUTHORIZATION TO RELEASE MEDICAL RECORDS ...

Releasing Protected Health Information
Medical Records Release Form in Word and Pdf formats
Medical records release authorization forms are documents which are intended to be filled out and signed by patients or individuals who will Fertility Center Medical Records Release Authorization Form - There are four sections in this type of medical records release authorization form. Patients or representatives with power of attorney can authorize release of Please submit your medical release form to the medical records office by fax, mail or in person. DISCLAIMER: The medical forms, charts, and other printables contained on FreePrintableMedicalForms.com are not to be considered as medical or legal advice.
