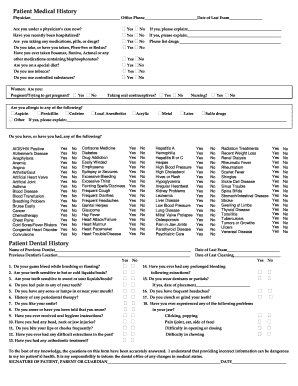
Patient Medical History Questionnaire Template. Fill, sign and send anytime, anywhere, from any device with pdfFiller. Upload the template, or select one from the PDFfiller.

Job applications and medical history forms, among others, are examples of questionnaires that have no intention of being statistically analyzed.
A large percentage of the time, you will actually be able to make a diagnosis based on the history alone.

Health History Questionnaire Template - Word Excel Formats

10-11 patient history forms templates - lascazuelasphilly.com
67 Medical History Forms [Word, PDF] - Printable Templates
10+ Patient Health History Questionnaire Templates ...
FREE 9+ Sample Health History Templates in PDF | MS Word

The Analysis of Medical Discourse Community - wiki.sdstate.edu
General Medical History Forms (100% Free) - [Word, PDF]
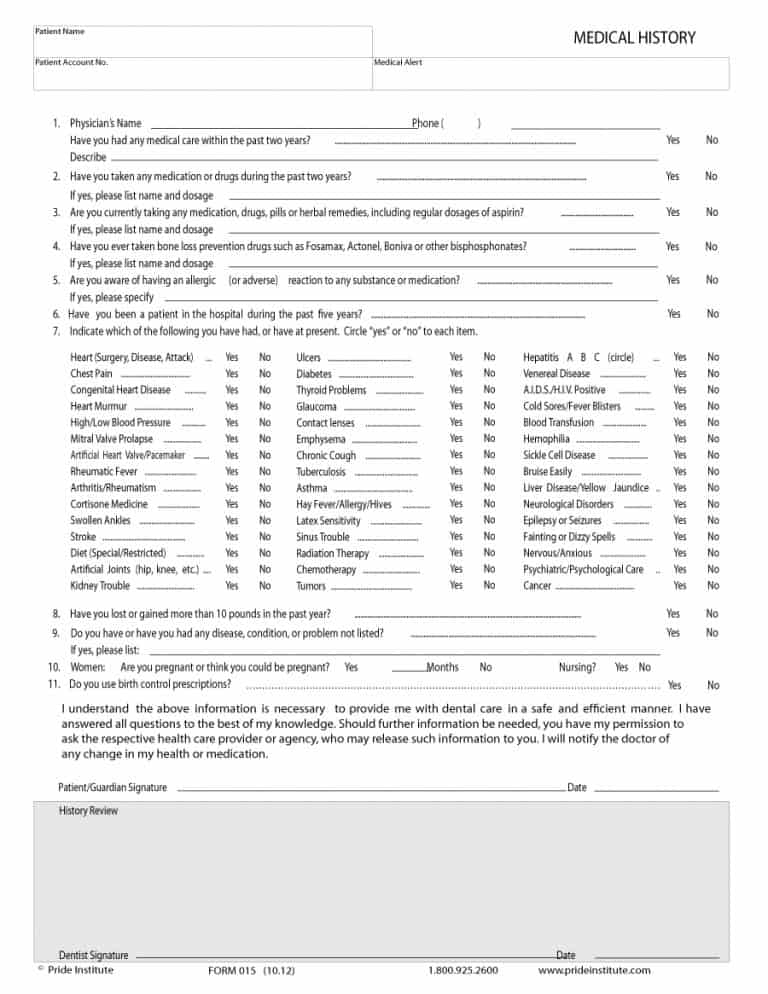
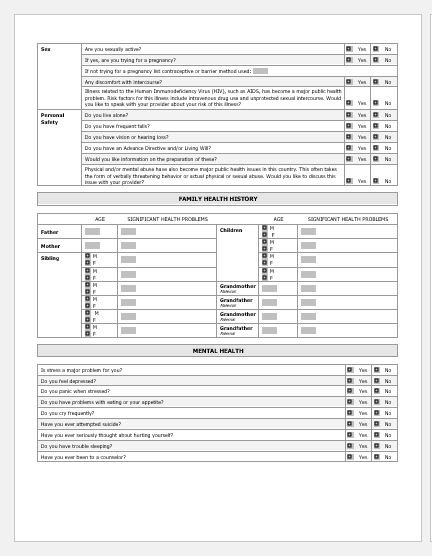
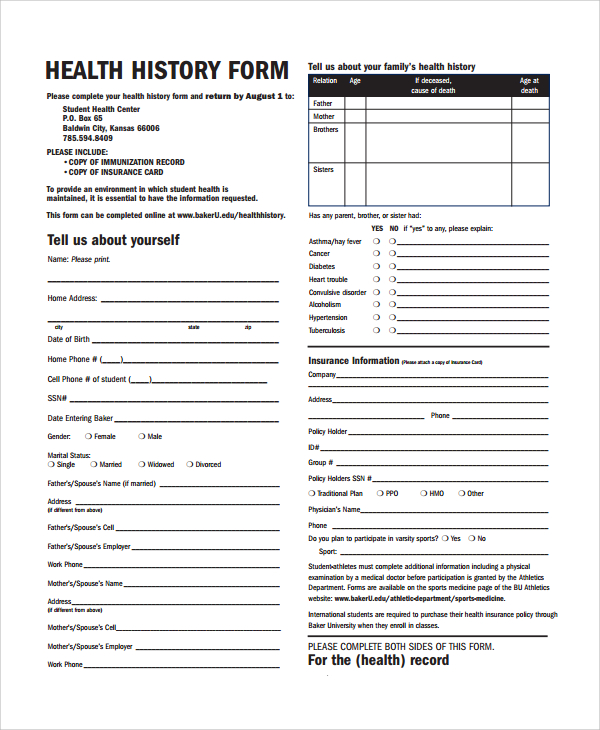
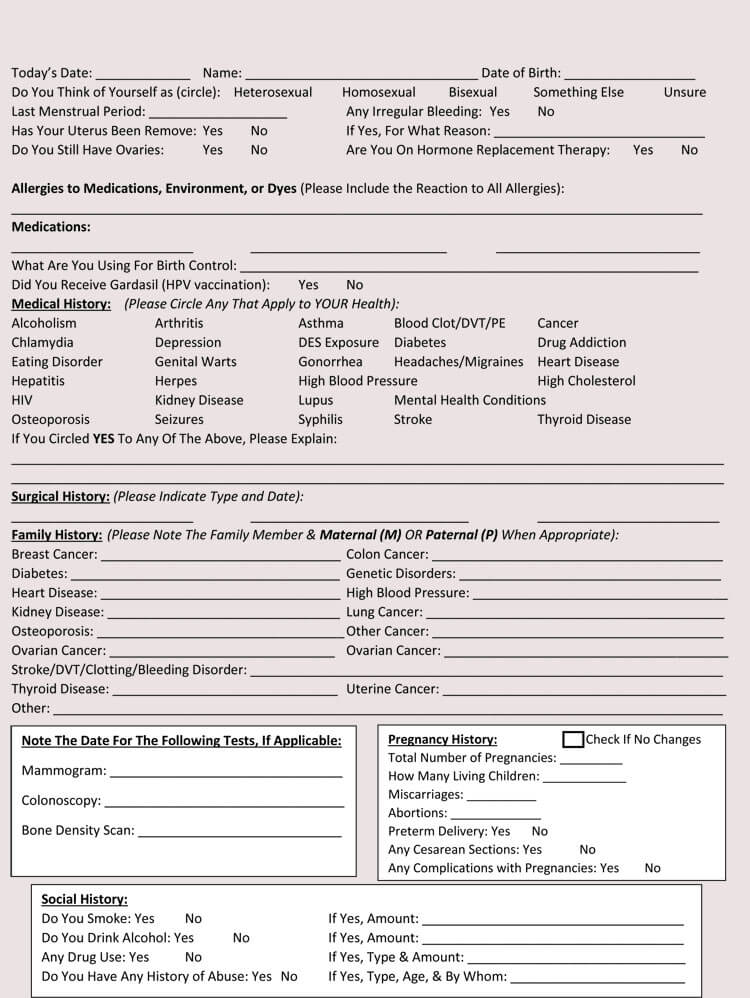
Get And Sign Patient Medical History Form (PDF) - Dental ...

Medical History Form - 9+ Free PDF Documents Download ...
There is no validated questionnaire to collect patient medical / medication history. Condition Skin Condition (Psoriasis) Skin Condition (Abnormal Moles) Sleep Apnea Stomach Ulcer Stroke Thyroid (Nodule) Thyroid High (Overactive). From the medical records available, is there any medical.
